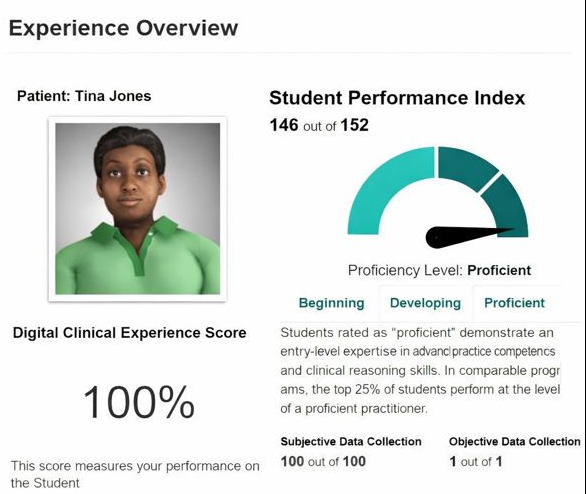
One of the core nursing skills that direct the process of assessment, care planning, and patient communication is a comprehensive health history. Tina Jones’s scenario of Shadow Health is a perfect example that demonstrates that. Nursing students have an opportunity to exercise structured health histories, which strengthen the skills of clinical reasoning and documentation. Health history begins with chief complaints, which include the origin of the problem, its intensity, and any related symptoms. The case of Tina Jones raises respiratory and endocrine issues, which helps nurses investigate the pattern of symptoms and triggers in a systematic way. The nurses are taught how to differentiate between subjective reports of patients and objective observations to ensure that data is collected accurately.
It’s important to also note that Tina Jones’ Shadow Health focuses on recording previous medical history, medications, allergies, family history, and lifestyle, which constitute the key elements of holistic care. Nurses train to become more familiar with the psychosocial and functional aspects of health, such as sleep, nutrition, and activity levels, as they occur during actual clinical encounters. Categorizing data into systematized forms, records, SOAP notes, or health history templates helps make sense of and improve the process of interaction. The case of Tina Jones illustrates the importance of documenting both the presence and absence of findings; for instance, no history of increased thirst as a negative finding would be important in a health history assessment since Tina Jones is a diabetic. It is important to apply these evaluations to make effective clinical judgments. Within a system of regular practice of health histories using structured cases like Tina Jones, nursing students can increase their critical thinking, make judgments in documentation more accurate, and gain confidence in their ability to conduct patient-centered evaluations.