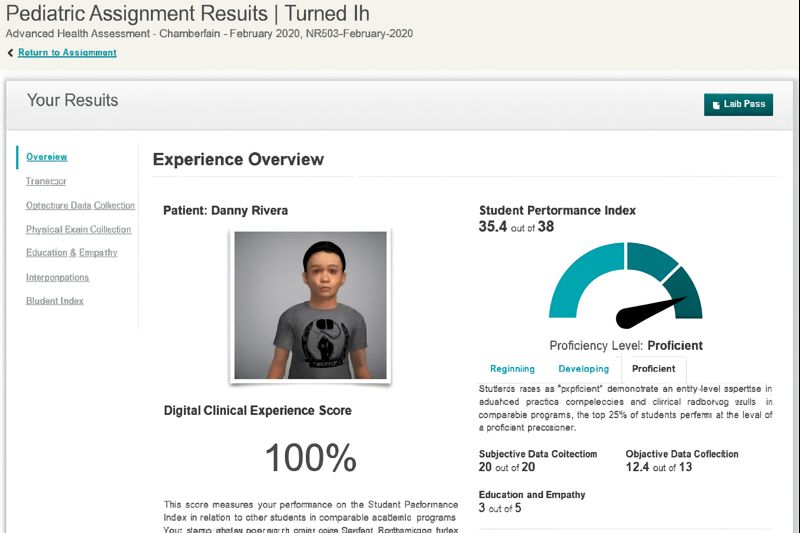
Precision, clarity, and clinical reasoning are essential in the documentation of pediatric findings in Shadow Health to reflect the practice in the real world. In the focused examination, Danny Rivera’s cough is reported as persistent, accompanied by related respiratory complaints. The assessment will ask the learners to gather a comprehensive health history, perform a dedicated respiratory exam, and combine the subjective and objective information to create the precise clinical image. Even though the case is virtual, it challenges nurses to identify subtle subjective information through conversational interactions and therapeutic communication with the patient, just as they would with a real pediatric patient. Detailed documentation starts with an articulate summary of the chief complaint, its onset, duration, nature, and related symptoms like the presence/absence of wheezing and shortness of breath.
The objective results of inspection, auscultation, and vital signs should be reported in professional language to mirror clinical findings. Professional pediatrics documentation, regardless of the Electronic Health Record (EHR) or a SOAP note, must integrate subjective and objective information into a logical story that facilitates clinical reasoning and the development of nursing diagnosis. The quality of documentation has a direct impact on the possibility to justify clinical judgments, suggest interventions, and organize follow-up care. Concise, evidence-based terminology uses a minimum of words, and still, it enhances the continuity of care in the event a future clinician is reviewing the record. The best pediatric documentation also includes caregiver education, response to teaching, and communication difficulties. Assessing the strengths and weaknesses of the documentation is crucial because it develops essential clinical thinking skills that will be applicable in real-world practice and future nursing documentation examples throughout your academic and professional life.